- Home
- Staying Connected
- GFF K&L Shares
- Officier de Liaison du GFF Post
March 29, 2022
|
01:36 PM
Innovations for demand generation and supply of Family Planning in Nigeria
 by Global Financing Facility Knowledge & Learning Platform
by Global Financing Facility Knowledge & Learning Platform
 Umma Yaradua has been the Liaison Officer for the Global Financing Facility in Nigeria 2016, providing support to the Nigerian government as it implements its RMNCAH+N Investment Case. She has worked across areas of public policy, governance, private sector engagement and health systems. Her main background is in clinical medicine, with training an Obstetrician and Gynecologist.
Umma Yaradua has been the Liaison Officer for the Global Financing Facility in Nigeria 2016, providing support to the Nigerian government as it implements its RMNCAH+N Investment Case. She has worked across areas of public policy, governance, private sector engagement and health systems. Her main background is in clinical medicine, with training an Obstetrician and Gynecologist.
Innovations for demand generation and supply of Family Planning in Nigeria
In approving the FP2020 blueprint the Minister of Health Dr Osagie Ehanire was quoted as saying
“Many cultures in Nigeria have names depicting the agony, dejection and the despair that come with repeated maternal and child death:” Ajuji” (i.e “child meant for rubbish dump”) among the Hausas in the North; “Abiku” (i.e “child predestined to die”) among the Yorubas in the South-West and “Onwubiko” (i.e “please death spare this one”) among the Igbos, for example. Each year in Nigeria, an estimated 33,000 mothers die, three-quarters of which could have been prevented with existing health interventions; 946,000 of children under five dies; 41,000 new-borns die, 70% of which could have been prevented using existing health care packages. This means that a total of about 1 million women and children die in Nigeria each year, equaling about 3,000 deaths per day and 2 per minute. We have an obligation and opportunity to change this situation, and a pivotal intervention is Family Planning.
Nigeria has a rapidly growing population of over 200 million, of which 46 million are women of reproductive age. With a total fertility rate (TFR) of 5.3, a low modern contraceptive prevalence rate of only 12% and a high level of unmet needs for family planning, NDHS reported 48% among sexually active unmarried women and 19% among currently married women. Nigeria is bound to continue breeding a highly dependent young population, consisting of children under the age of 15 making up 40% of the population (See Figures 1). The unmet need for family planning is disproportionately accentuated among younger women, those in rural areas, with less education, and in lower wealth quintiles. This is partially due to the lack of knowledge, as well as strong cultural factors.
Figure 1
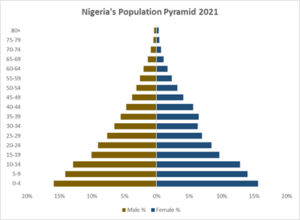
Source: National Population Commission, Abuja Nigeria (July 2020). Nigeria Population Projections and Demographic Indicators
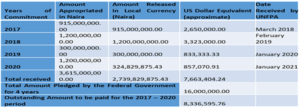
Provision of Family planning (FP)commodities in Nigeria has been largely donor driven, mostly by FCDO, Canada and UNFPA from 2003 to 2011. In line with the FP2020, Nigeria in 2017, committed to paying $4Million annually for the procurement of FP, from 2017 to 2020. Unfortunately, the country has not kept up its side of the bargain (see Table 1).
Table 1: Government Counterpart Contributions for Commodity Procurement Approval by Federal Executive Council for 2017 – 2020 @ USD4,000,000.00 Per Annum (@ $1 = N345)
According to a study done by the Guttmacher Institute, if all unmet need for modern contraception in Nigeria were satisfied, unintended pregnancies would drop by 77%, from 2.5 million to 555,000 per year.[1] As a result, the annual number of unplanned births would decrease from 885,000 to 200,000 and the number of abortions would drop from 1.3 million to 287,000. Expanding contraceptive services help offset the cost of improving pregnancy-related and newborn care by reducing unintended pregnancies. For every US$1 spent on contraceptive services beyond what is currently spent, we would save US$2.77 in the cost of improved maternal, newborn and abortion care. In 2016, states governments allocated the sum of US$7,052,480 in matching funds for the family planning programme through the IDA loans disbursed through the Saving One Million Lives (SoML) project and NSHIP project.
In 2011 following strong advocacy to improve access, the GoN decided to make FP free in all PHCs and some private facilities. But despite this, mCPR is still flat (See Figure 2), as State governments who are responsible for getting the products to the clinics, pharmacies etc., from where the women can access them don’t have financing to make this happen.
Figure 2

| Supply side barriers include
1. Cost of FP commodities (FP is provided free in public facilities but at a cost in private facilities) 2. Lack of manpower to provide services 3. Capacity to provide effective and efficient services 4. Opening and closing hours of the facilities 5. Availability of commodities 6. Procurement difficulties – major stock outs across facilities 7. National – low government commitment at all levels, Poor availability of youth-friendly information channels and services |
The Federal Ministry of Health revised National Family Planning Blueprint (2020-2024), which aims to increase the modern contraceptive prevalence rate (mCPR) from 12% in 2018 to 27% by 2024. This represents a projected 3% annual increase from the present national mCPR[2], estimated to cost US$252,004,187. These costs are expected to cover the period of the FP Blueprint, with costs of commodity increasing over time as more women are reached. Demand for FP is a huge barrier to the access, which has resulted in demand generation as part of the programming.
Demand generation activities aim to increase clients’ desire to use family planning by changing their attitudes or perceptions about FP or increasing their awareness or knowledge, including social and cultural norms about FP methods. In a country as big as Nigeria, innovative ways to increase demand and uptake is key not only for the women and girls but also for our national development to help reduce maternal and under 5 mortalities. Based on the FP blueprint, of the $252 budgeted only $3.5 Million will be used over the years to address issues around demand generation, with the largest amount going to procurement and supply chain management. This figure is estimated to be less due to the current FCDO cuts that will affect many LMIC countries, of which 28 are GFF countries and made worse because of the Covid-19 pandemic.
| Demand side barriers include
· Individual Level – fear of side effects, myths, and misconceptions about modern FP. · Family Level – desire for large families, spousal opposition, low socio-cultural position of women · Community Level – low awareness among traditional/religious leaders, FP provider bias · Difficulty accessing services from the facilities · Non-availability of transport – worsened during the lockdowns |
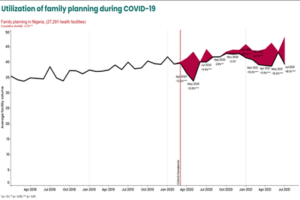
Over 76% of PHCs were providing RMNCAH services including family planning3. Due to the lockdown, there was a decline in assessing services with wide variations across and within States because of COVID-19.[3] Without efforts to mitigate poor access to services, it is estimated that between 357,000 and 1,420,000 women could be unable to use contraception resulting in 8,920 to 425,000 unintended pregnancies in Nigeria.[4] Pentavalent 3 doses fell by 14% in April, and recovered to expected levels as of September 2020, on analysis of the DHIS2 ( see Figure 3)
Figure 3
Why is this Important
Nigeria’s population is likely to hit 379 million by 2050, becoming the fourth most populous country on earth. High fertility rates because of desire for large family and low FP uptake are major factors in Nigeria’s rapid population growth. Without efforts to curtail the growth in population the country is headed to a demographic disaster – as already seen in economic, social, and environmental challenges the country is currently facing every day. Bold steps need to be taken to address not only FP but sectors like education, health, women empowerment, and productivity.
Innovations to improve uptake of FP
As the current uptake of FP services is low – due to both demand and supply challenges, innovative ways to address these must be introduced especially now during Covid19 when there is a reduction in accessing essential health services. This can be seen from the use of ICT and the use of different applications to support the availability of public services[5] in Indonesia during the pandemic.
Demand side innovations
- Family planning communication plan using dots was adopted by the states in 2017 – The National Family Planning Communication Plan (NFPCP) spells out the steps to rebranding of Family Planning services through the official launch and presentation of the NFPCP and the New National FP Logo “The Green Dot” will generate public discussion and assist Nigerians to locate where they can get quality, safe and trusted Family Planning services in both public and private health facilities across the country.
- Community outreaches to provide information, counsel and provide services and referrals, Self-taught using the injection Sinepress directly provide 1-year free supply (useful in pandemic)
- Ongoing efforts to strengthen community-based family planning programs in collaboration with NPHCDA to buy into CHIPS program
Supply side innovations
The covid-19 pandemic provided a huge opportunity for innovative thinking around the world. The Ministry of Health had to come up with innovative ways to maintain essential health services especially family planning in collaboration with partners, the civil society, and the private sector.
Sixty percent of women access FP through the private sector, more so during the pandemic[6] . Nigeria developed a task-shifting task-sharing policy for essential health care services in 2014 which was updated in 2018, and one of the aims of this policy was to enable community pharmacists and patent and proprietary medicine vendors (PPMVs) provide services including FP. Currently 22% of women receive their FP commodities from the PPMVS[7] especially for adolescents and young people (15 to 24-years-old). This approach is like the one done in Kenya where the Pharmaceutical Association and the Ministry of Health worked together to build the capacity of pharmacy staff on available contraceptive methods, counseling youths and establishing an effective referral system. In Nigeria, partners have lent their support for this agenda through:
- The GFF – to develop guidelines to help maintain essential health services through “the Policy dialogue on engaging patent and proprietary medicine vendors (PPMVs) in the provision of essential health services, commodities during the covid-19 pandemic and other infectious epidemics”.
- The Integrate project, implemented by a consortium led by the Society for Family Health (SFH) with funding from MSD for Mothers and in partnership with the Bill & Melinda Gates Foundation has, since 2017, been working with the Federal Ministry of Health (FMoH) to broaden its task-shifting task-sharing (TSTS) policy. This is being done by piloting a system led by the Pharmacists Council of Nigeria, to test a model in Lagos and Kaduna with the view to scale up to other states. It aimed to improve access and uptake of family planning services with the overall objective of improving contraceptive coverage.[8]
On the other hand, government has also put some measures in place to improve supply of FP commodities and quality of services.
- Community Health Extension Workers (CHEWS) – they distribute door to door and to the facilities (e.g., pills, sinepress). Strengthen community-based family planning program to ensure that FP clients receive services and commodities within their immediate communities including in humanitarian settings. Web-based & Online in-service Training Methods adopted.
- FP Commodity supplies & Services are being integrated into the overall National Health Response to Covid19.
*********************
[1] https://www.guttmacher.org/fact-sheet/adding-it-up-contraception-mnh-nigeria
2 Nigeria Family Planning Blueprint 2020- 2024 accessed from https://health.gov.ng/doc/final-2020-Blueprint.pdf on28th April,2021.
[3] Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: a cross-sectional study – Adelekan et al. Reprod Health (2021) 18:166
[4] Maintaining Access to Contraceptives During COVID-19 Disruptions – Potential impacts and mitigation in Nigeria
[5] Innovation in Coping with the COVID-19 Pandemic: The Best Practices from Five Smart Cities in Indonesia – Rini Rachmawati et al Nov 2021
[6] Mitchell, S. 2013. “The Role of the Private Sector in Family Planning.” Blog. November 10. http:// healthmarketinnovations.org/blog/role-private-sectorfamily-planning. Accessed June 7, 2017
[7] National Population Commission (NPC) [Nigeria] and ICF. 2019. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF
[8] Integrate Private Sector Providers to Improve Access to Family Planning Commodities and Services – Jan 2022